


A World Where There Are No Boundaries To A Healthy Future For All

Thirty-six years ago today, the space shuttle Challenger exploded 73 seconds after liftoff. Like many children of the 1980s, the Challenger shuttle launch was a big deal for me because one of the seven astronauts was a teacher, and she was planning to conduct two lessons live from space. As a curious kid with an imagination that stretched to the stars, the thought of learning from a real-life astronaut in space was thrilling. I remember where I was (2nd-grade Central Elementary School) and who told me about the explosion (the substitute Mrs. Huber, not my real teacher, who was also Mrs. Huber). I remember she cried as she told us. I remember watching the launch and explosion on the local news several times that evening with my family. I remember President Reagan talking to me and all the other American children that night, as we mourned our loss of innocence.
The Challenger disaster was the defining tragedy of my childhood.

I often highlight the Challenger disaster in my classes when talking about statistical correlation and statistical errors. NASA engineers knew that the O-rings/seals (which are responsible for maintaining the internal pressure of the rocket boosters) were not as effective at colder temperatures (compared to warmer ones). The night before the Challenger launch, temperatures in Florida were below freezing and a decision had to be made about the robustness of the O-rings. The statisticians built a model to predict if a successful launch was possible with the existing data. Unfortunately, the coldest temperature for which data was available was 54*F.

The model they created was out of range for the real-world launch conditions. And it is clear that the line-of-best fit used to predict the number of O-ring failures could not accurately predict what would happen at temperatures below 40* using temperature data that ranged from 54-81*F.
Correlation does not mean causation.
Even though we can draw the line-of-best fit, it does not mean that it is predictive of what is going to happen. And the range of real-world data must be used to create a context within which conclusions about that line can be made. It is definitely not one-size-fits-all.
In addition to this, leaders at NASA only looked at selective data when making their decision to launch the Challenger. Specifically, they looked at the table below — which included only data about the O-ring failures. You’ll see when looking at just failure data, the decision-makers saw that O-ring failures happened across the range of temperatures (from 54-75*F), which led them to conclude that launches at 36*F would not put the structure of the solid rocket boosters at increased risk.
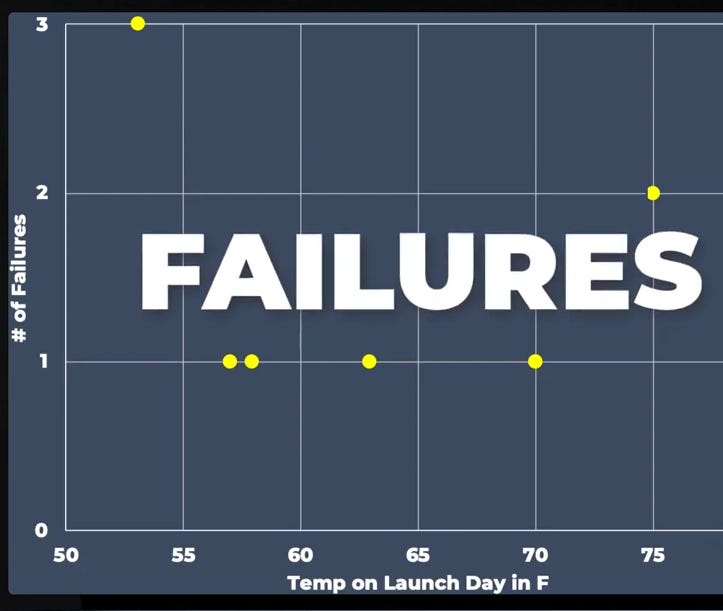
However, looking at the full set of data — both when there are O-ring successes and failures — it is clear that the O-rings do not function properly when temperatures drop below the mid-60s; sixteen launches that occurred above 65* resulted in zero O-ring failures. Seeing that zero O-ring failures occur in warm temperatures helps one to understand that risk of failures increases at lower temperatures.

Looking at selective data leads to flawed decision-making.
I believe the Challenger disaster has many things to teach us as we make our way through the Omicron outbreak of the COVID-19 pandemic.
First, related to statistics — when making individual or policy-level decisions about vaccinations, masking, closures, we need to look at all of the data. Three common mistakes I hear people making include:
A friend of a friend died from the COVID vaccine; when in fact the death followed the vaccination. Unfortunately, people do die (we all do, actually). And just because an individual dies after receiving their COVID vaccine, it does not mean that their death was caused by the vaccine. Correlation does not equal causation. According to VAERS, there have been 11,657 reports of death (0.0022%) among people who received a COVID-19 vaccine. However, these are just reports. And each death needs to be investigated to determine if the vaccine was actually the cause of death. The order of events (the timeline — vaccine followed by death) does not mean the vaccine caused the death.
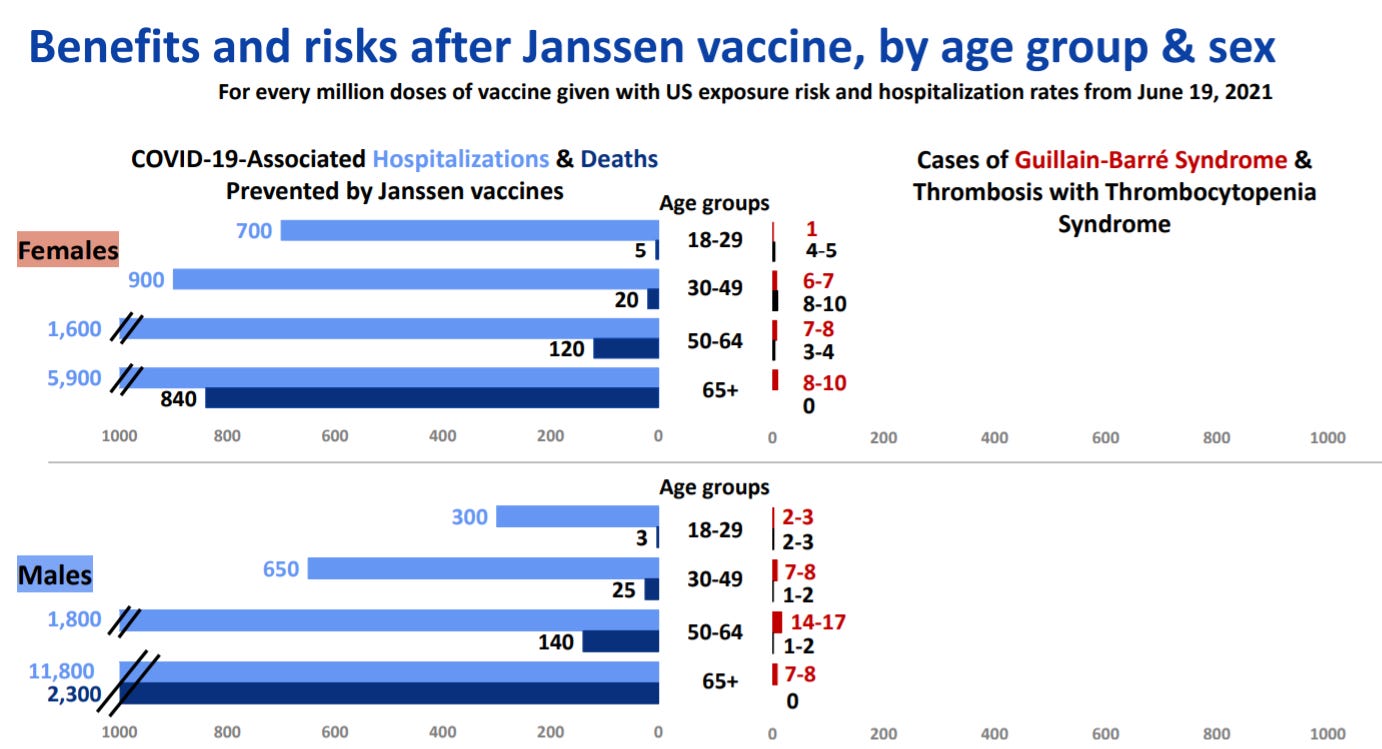
Deciding not to get vaccinated because there are adverse events associated with the vaccine. For example, there is a minimal risk of Guillian-Barre syndrome (GBS) associated with the J&J vaccine. If one looks at just the number of GBS cases associated with vaccination, they may decide not to get vaccinated (no one wants GBS). However, there is a lot of data associated with not getting vaccinated (severe disease, hospitalization, and death). We must look at the risks of the vaccine as well as the benefits of it in order to make a decision about getting vaccinated or making a policy about vaccinating.

When looking at all of the data, the risks associated with COVID infection (in blue) far outweigh the risks associated with the vaccine itself (red/black).Declaring that schools, especially K-12, should go remote in the midst of the Omicron surge. While I haven’t come out and said it yet, (here goes)
I am very much opposed to remote education even in the midst of Omicron.
With the accessibility of vaccines for everyone ages 5 and up, the protection provided by masks, and the reality that Omicron is less virulent (or causes less severe disease), I believe we can create a safe in-person learning environment. [Note: this does require that all of our teachers are vaccinated and boosted, masks are worn, and sick individuals are required to stay home for at least 5 days.]
And COVID is only one piece (a big one) of a healthy school system. We know (especially for the little ones) that remote learning cannot replace in-person instruction. Additionally, schools provide students with meals, warmth, positive adult mentors, and so much more. When schools shifted to remote learning, the number of reports of child abuse decreased and the mental health of our kids got a lot worse.
We have learned so much about preventing and treating COVID during the past two years. We have amazing vaccines that are available to all K-12 students. We know masks work. We know that keeping sick kids out of school buildings decreases the spread of disease. We have amazing test-to-stay programs that provide frequent testing to ensure that asymptomatic kids are not in school while they are infectious.
The benefits of learning in-person learning (with all the mitigation strategies in place in the middle of Omicron!) far outweigh the COVID risks in schools. When we look at all of the health data related to kids and schools — COVID data and all the other public health surveillance and survey data — my conclusion is we need to keep the doors open and kids in the classroom.
Following the Challenger disaster, NASA was forced to pause the shuttle program and rebuild. And while we cannot completely pause life in the middle of the pandemic, we can think about rebuilding; creating healthy communities for all.
Public health (much like NASA in the 1980s) has been underfunded and overworked for decades. The pandemic has brought to the forefront the limitations of an underfunded and exhausted public health workforce.
It is time we valued our health care as well as our community/public health.
Christa McAuliffe, the teacher who died aboard the Challenger in 1986, risked everything to be part of scientific exploration to make a difference for the future for all of us. I think it is time we all follow in her footsteps — to take risks, advocate for, dream of, and put together a public health system that will ensure a healthy future for all of us. Before her 73 second flight on Challenger, Christa McAuliffe said —
“I have a vision of the world as a global village, a world without boundaries.”
I hope we can build on her vision for this global village —
to create one in which there are no boundaries to a healthy future for all.
Your description of "SAFE in-person learning " is so important but, sadly, not happening. Thank you for all your clear information.