

The J&J PAUSE continued...
The J&J PAUSE continued...
More data needed before making a decision about the J&J COVID-19 vaccine

Yesterday the Advisory Committee on Immunization Practices (ACIP) met to discuss the occurrence of rare blood clots (a severe side effect) associated with the J&J vaccine. Simply put the meeting centered around the question — should we end/limit the use of the J&J vaccine because of this rare, but severe side effect?
After a thorough review of the data, public comments, and discussions, including presentations from J&J and the ACIP subgroups focused on vaccine safety and the COVID-19 vaccines, the ACIP decided more information is needed in order to make a decision (read: vote) about the use of the J&J vaccine.
This means that until further notice the J&J vaccine will NOT be distributed or administered to individuals in the United States.
Here is what we learned and what was discussed during yesterday’s ACIP meeting —
Approximately 7.5 million individuals worldwide have received the J&J vaccine (343,000 received the vaccine as part of the clinical trials and studies + 7.2 million who received their dose after the vaccine was approved). There have been 9 cases of CVST with thrombocytopenia (low platelet counts). This is a specific type of blood clot where blood in the brain cannot drain properly (in a vein) and this results in a brain bleed. These clots are combined with low platelet counts, which means heparin (a common treatment for clots) cannot be used to treat the individual and the patient can have fatal internal bleeding.
Six of the cases occurred among individuals who received the J&J vaccine after the Emergency Use Authorization was issued, one has died and another is currently hospitalized. We know that one of these individuals was on birth control (which increases the risk of blood clots) and none had a pre-existing coagulation disorder.
In order to assess whether these cases of CVST with low platelet counts were associated with the J&J vaccine (meaning we see more cases among those receiving the vaccine compared to those not receiving the vaccine), rate ratios were calculated. A rate ratio is a comparison between the rate of CVST with low platelet counts among those receiving the vaccine compared to (or divided by) the background/before J&J vaccine rate of CVST in the population.
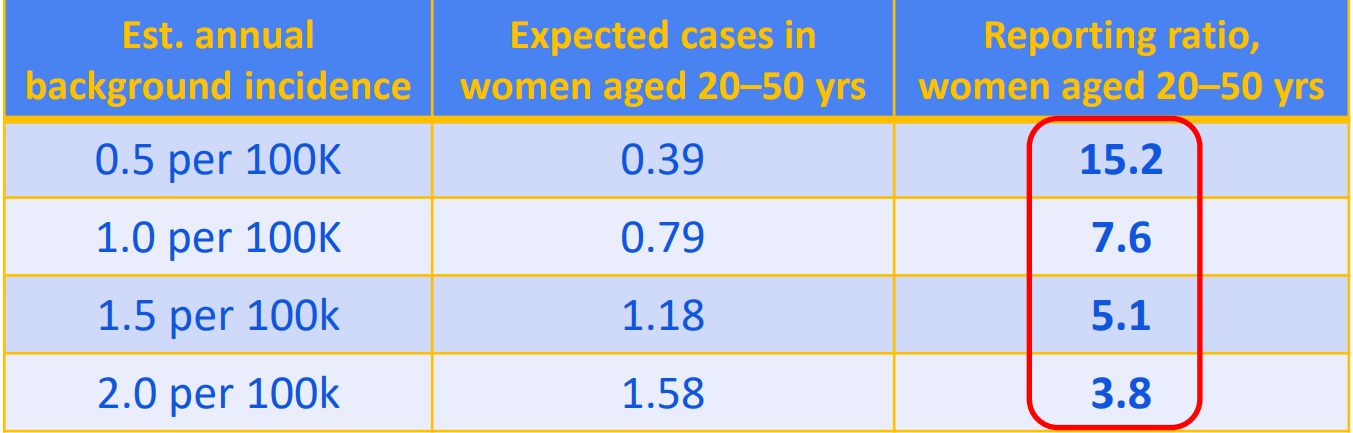
In the table above, we see that the “background incidence” or the rate of new cases of CVST per 100,000 people ranges from 0.5-2.0 (seen in the first column, Est annual background incidence). NOTE: this is the rate of CVST regardless of platelet count. CVSTs are rare and CVST with low platelet counts are even rarer. The findings highlighted above and discussed below are conservative or underestimates of the risk of CVSTs with low platelet counts associated with the J&J vaccine.
The column with the red circle tells us the increased risk of CVST with low platelets among the vaccinated group compared to the background rate of CVST (with and without low platelets). The interpretation of this data is that those who were vaccinated with the J&J vaccine have a 3.8-15.3 fold increase in the risk of CVST compared to the background rate. This is a KEY piece of epidemiological evidence (pointing toward causality) as we investigate whether or not the J&J vaccine causes this severe side effect.
The ACIP decided to continue to pause the distribution and administration of the J&J vaccine for the following reasons —
More than 50% of the J&J shots administered in the U.S. were given between March 30 - April 12, meaning there is another cohort that is still in the window (~3 weeks post-vaccination) of being at risk for this serious adverse side effect.
To continue communications with clinicians — we need to ensure clinicians who have patients reporting symptoms associated with this side effect know how to treat these individuals, know to ask if they have received a J&J vaccine, and know how to report the adverse effect to CDC.
We need more data. Specifically, the rate of the occurrence of these rare blood clots is needed by sex and for different age groups. Comparisons between the rate of CVSTs in the vaccinated group compared to the background levels are needed. Additionally, we need to know how often blood clots occur among COVID+ individuals and how that rate compares to the rate among those who are vaccinated (we want to know: are you more likely to get a clot from COVID or the vaccine?).
A full risk vs. benefit analysis is needed to determine if the benefits of the J&J vaccine out-weight the risks and for whom.
While this PAUSE is a huge blow to the global vaccination effort, there is a silver lining. Our public health surveillance systems that track these adverse side effects work. And the data/science was prioritized to make the best decisions to ensure safety (the original pause on April 12 and the continued pause decision from yesterday). The ACIP members stated again and again during yesterday’s meeting that their job is to use the data to make decisions that will “do no harm.”
There are real concerns about continuing the pause on the distribution and administration of the J&J vaccine — first, using the J&J vaccine to vaccinate hard-to-reach groups with limited access to health care (migrant workers, the homeless, and those who are home-insecure) was a priority. Using a single-dose vaccine that does not need to be stored in a deep freezer was the ideal situation to increase vaccine uptake within these groups. Pausing the J&J vaccine will mean there will be limited access to the vaccine within these groups. Additionally, while ACIP’s jurisdiction is limited to the U.S., the opinions and decisions of the ACIP are respected worldwide. The pause of the J&J vaccine in the U.S. could result in other countries who only have access to the J&J vaccine pausing their vaccination programs at this time - bringing a complete stop to their vaccination programs. And slowing the global vaccination process.
What’s next?
The Pfizer and Moderna vaccines will continue to be used in the United States. CDC, FDA, and J&J are working collaboratively to collect and analyze the data requested by the ACIP. So… we all wait. And we pray that no additional cases of CVST with low platelet counts arise from the group that was vaccinated with the J&J vaccine during the last three weeks.
The ACIP will meet as soon as possible. Updates and summaries will be provided here.