
Anatomy of the Mask Trial
Key takeaways & applications from the mask study conducted in Bangladesh

On September 1, the results of the first (and very large) trial to assess the impact of mask-wearing on the spread of COVID-19 were shared online. (It feels like) Everyone is talking about the results. And I’ve been thinking about this study A LOT for two reasons - first, the study clearly shows that mask-wearing reduces the spread of COVID-19. And second, this study provides a great opportunity for me to teach you how to read, assess, and apply the findings from epidemiological research.
So settle in as I walk you through the anatomy1 (the study of the form & function) of a randomized controlled trial focused on mask-wearing in Bangladesh.
Epidemiological papers begin with a background/introduction to help bring the reader up to speed on the topic at hand. For this paper, the authors start by saying (hey!) a lot of epidemiological studies have been done and they all demonstrate that masking decreases the spread of the SARS-CoV-2 virus. However, the authors point out that there is something missing in this body of evidence -- a randomized trial (which is the gold standard in medical/public health research) demonstrating the effectiveness of mask-wearing has not been done.
Through a collaboration, researchers at Yale and Stanford joined forces with several groups in Bangladesh to complete a multiple-month randomized controlled trial that included more than 340,000 individuals. One of the main goals of the study was to examine the effectiveness of masks in reducing SARS-CoV-2 spread in a real-world setting. The anatomy of the study design (read: the methods used) looked like this --
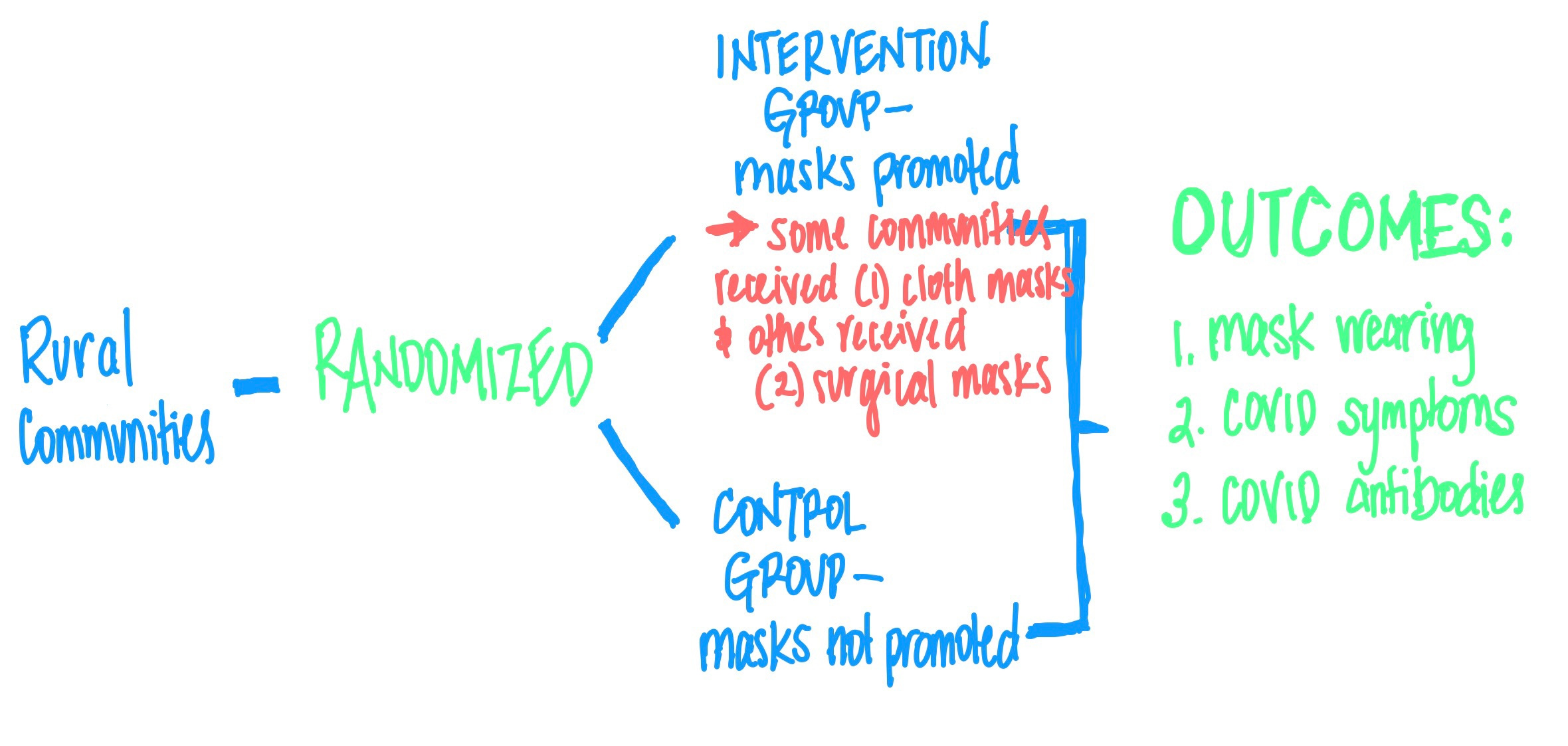
Since substantial transmission of COVID-19 stems from asymptomatic or pre-symptomatic individuals, the process of randomizing the villages (not individual by individual) allowed for an assessment of the full impact of masks on COVID infections, including the transmission of the virus from person to person.
The authors found that increased mask-wearing resulted in a significant reduction in the percent of people with symptomatic COVID-19. To quote one of the researchers, Dr. Laura Kwong --
“These results suggest that we could prevent unnecessary death and disease if we get people to wear high-performing masks, such as surgical masks, in schools, workplaces, shopping centers, places of worship, and indoor spaces.”
Specifically, the study showed that mask-wearing caused an 11.9% reduction in COVID symptoms. NOTE: this does NOT mean that masks are only 11.9% effective. What this means is that we see a ~12% reduction in COVID symptoms among people in the intervention/mask group compared to the control group. Additionally, there was a ~10% reduction in individuals with COVID symptoms who were also seropositive for COVID antibodies. This means that masks work well to prevent COVID transmission, but they also prevented people from experiencing symptoms caused by other respiratory diseases.
This is all good news. Actually very good news. Given that the transmission rate in Bangladesh was low during the study period (only 2-3% case positivity) and that in the intervention group fewer than 50% of people wore their masks, the impact of masking on disease spread will increase as more people wear their masks. It has been noted that these results are likely --
“the minimum effect of mask-wearing in a community.”
Masks work to prevent the transmission of COVID.
But what about surgical versus cotton/reusable masks? Not surprisingly, the research team found that (high-performing) surgical masks were better at preventing the spread of COVID-19. Cloth masks did prevent transmission, but the evidence was not as strong or statistically significant as the surgical mask evidence was.
So what does this mean in terms of public health and our individual mask-wearing behaviors? First and foremost, the time for debating whether masks work at slowing the spread of COVID-19 is over. Masks work to prevent the transmission of COVID.
Should you wear a surgical mask? or a reusable mask?
Honestly, I think it depends. Here is the list of questions I’m using to help my family navigate our mask-wearing decisions…
Is anyone in your immediate family (or quaranTEAM) at high risk for severe COVID?
If so, surgical masks are recommended to provide that person or the mask-wearer with the most protection.Is the mask wearer vaccinated?
I’m more likely to let my vaccinated 12-year-old wear a cotton mask than my unvaccinated 9-year-old. He does not have the protection of vaccine-induced immunity; so I’m extra cautious with him.Where are you going?
Here in Pennsylvania, there is a mask mandate for K-12 schools - I am more likely to allow my kids to wear reusable masks to school because their classmates and teachers will also be masked. If I were going to teach in a setting without a mask requirement, I would be wearing a surgical mask to give myself the most protection possible (honestly, I’d double mask - surgical mask covered by a cotton mask).How high is the community spread in your area?
When the spread is high, switching to a surgical mask might be advisable.Do you know if the individuals you are going to be around are vaccinated? are many of them wearing masks?
Observing who is around you and the type of environment you are in is important. If you are going to a crowded stadium to watch a football game, I might choose to wear a reusable mask if I’m going to a stadium that requires everyone to be vaccinated (shout out to the Buffalo Bills!). But if I were going and vaccines were not required and most people were not masking, I would definitely wear two masks. (But who am I kidding… I’m not going to any big events!)
Ultimately, to quote Larry Gostin (a prominent public health lawyer) --
“Masking is a population-based blanket that we have to get widespread adoption of.”
As cases counts, hospitalizations, and deaths from COVID increase, we need to work together to slow the spread of COVID-19. The public health research community has provided evidence showing that masking works to reduce disease transmission.
This study did not show that masks stop (or end) the transmission of the virus. Instead, it showed that masks decrease disease spread and are an important tool in our collective work to end the pandemic. Masks combined with vaccinations and increased ventilation, smaller gatherings, and proper handwashing will lead to a decrease in disease spread (and ultimately the end of the pandemic).
Masks are not perfect. But masks will slow disease spread.
Our goal is -- progress over perfection.
Masks on!
I would guess that when most of us think about the word ANATOMY we think of human anatomy - the scientific study of the form and structure of the human body. For many individuals who work (or aspire to) in the medical field, studying anatomy is important; really important. In medical school, it is recommended that students spend upwards of 10-12 hours outside of class studying anatomy each week (essentially a part-time job studying the body). Anatomy is the hallmark of medical education.
As an epidemiologist - who investigates diseases in groups of people - I would argue that understanding the anatomy of medical research should also be the hallmark of medical education. Understanding how medical research is conducted, how statistics are used, how to properly design and power a study, how to discuss the strengths and limitations, research ethics, and (most importantly) how to apply medical research to improve human health - is a cornerstone of medicine as well as public health.