


Walking the Pandemic Tightrope
Stepping into 2022 with testing options changing, new isolation & quarantine guidelines, and the need to rethink what metrics we use

I feel like I am walking on a tightrope high above the ground.

To be clear, I can only imagine what it would feel like to walk on a tightrope across Niagra Falls. Shoot — I get nervous walking across the enormous and structurally sound Rainbow Bridge. Stopping to snap this picture nearly brought me to tears (that smile is as fake as can be; this moment was terrifying).

But as I think about the future — the new year and the 2nd anniversary of COVID-19, I think the image/feeling of walking on a tightrope is a useful metaphor.
We have been navigating a world filled with the SARS-CoV-2 virus for two years now (about 1 year and 360 days more than any of us expected or were prepared to handle). We are halfway across the falls on the tightrope. For many, their hands, hearts, and minds are numb. We are all (metaphorically) carrying a 40-pound balance bar full of emotions (namely frustration, fear, exhaustion, and loneliness). And the only choice we have is to take another deep breath (read: go to yoga) and then to (simply?!?!)
take
the
next
step.
We are all trying to balance our own physical, mental, emotional, and spiritual health; to make the best decisions in the midst of so much information and noise. The fog of social media, know-it-all-friends, and cable news makes it hard to see the rope, let alone our own feet (and if they are in fact still on the rope).
We cannot turn around and go back, but the end is nowhere in sight.
We must breathe, balance, and take the next right step.
As we enter year three of the pandemic, we must recognize that we are transitioning to a world that will include COVID forever. And with this transition, there are a lot of changes — changes to testing, quarantine & isolation, and metrics — occurring.
Testing
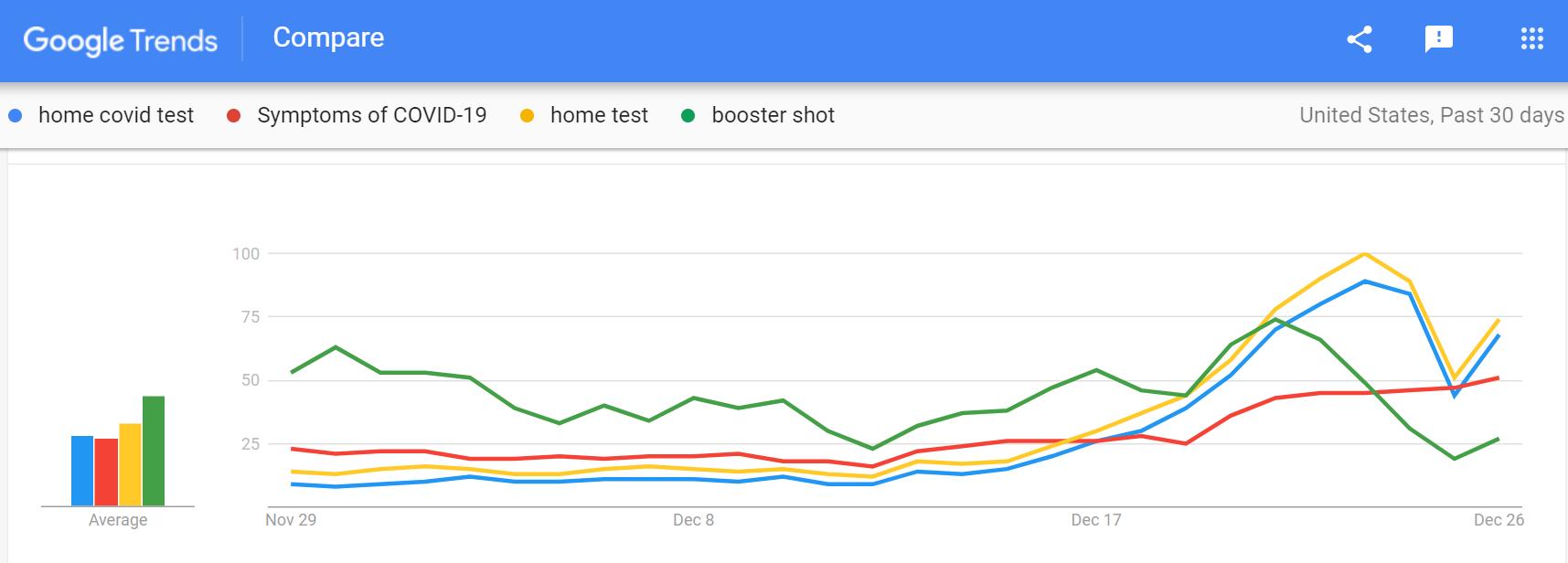
In light of Omicron —which is most definitely more transmissible than previous variants and likely causes milder symptoms (especially among the vaccinated) — and holiday travel, at-home COVID tests have become all the rage. Individuals can take a test to be sure they are COVID-negative before gathering with friends and family or to determine if their runny nose is an allergy or COVID infection. A google trends analysis shows that a lot of people in the United States were googling for “home test” during the past week.
Unfortunately, the demand for at-home tests FAR outweighs the supply right now. Amazon is anticipating the next shipment of tests will go out in mid-January.
Additionally (unfortunately), if an individual gets a positive result from an at-home test and does not follow up with a confirmatory PCR test, that case is not included in the daily count of positive COVID cases (more on this below).
Unfortunately (again), home tests are not affordable (on average a test costs $7-15), and they are not covered by insurance. As the supply increases and federal funds are used to make at-home tests more accessible and affordable (read: free), they will become an important tool for diagnosing COVID infections.
As we move into 2022, rapid test results are needed.
Free and accessible testing is needed.
At-home tests are needed to make game-day decisions about our health.
Quarantine & Isolation
On Monday, CDC updated and SHORTENED both the isolation and quarantine periods for COVID. Individuals who are boosted, are not required to quarantine following a known exposure to COVID, but those individuals must wear a mask (option to get tested, too). Those who are unvaccinated or not boosted, do need to quarantine. The quarantine period has been shortened to FIVE days. For anyone (regardless of vaccination status) who is diagnosed with COVID, if they are asymptomatic or symptoms are improving, the period of isolation was been shortened to FIVE days.

Many people have asked if I agree with these changes. I have A LOT to say and will save all my thoughts and questions for a separate post. Stay tuned…
Metrics
Since the beginning of the pandemic, we have used several metrics — the rate of disease per 100,000 people and the case positivity (a proportion) — to understand the amount of community spread of COVID, or put another way, to understand how common COVID is in a particular area. We’ve used the rate of hospitalizations and mortality to determine how severe COVID infections are in a community.
As we move into 2022 — with home tests being all the rage, shortened isolation requirements, and reinfections/breakthrough infections becoming more common — we can no longer rely on just our old metrics. Case counts, which are used to calculate the rate per 100,000 people are determined by PCR test results only. Home tests and rapid antigen tests are not included in those numbers. We know that the rate per 100,000 people is an underestimate of the true rate of disease (it always has been). But with at-home tests becoming more popular there is no system in place to track or count the number of people who are testing positive at home.
Even following the trends in the rate may be misleading. It is possible that a decrease in the case rate could be a reflection of an increase in home testing; not a true decrease in the number of infections. [Note: the case count — just PCR tests — across the United States has increased by 126% in the past 14 days. It is clear that community spread is increasing; Houston, we have a problem.]
Here is the reality — the public health surveillance system is broken. It needs to be rebuilt to include different sources of data, and it needs to be automated. We need to move the public health surveillance system into the 21st century.
Another common metric used throughout the pandemic to determine the level of community spread is case positivity (the number of positive COVID results divided by the total number of COVID tests administered). This number has become completely unreliable. In my county, the case positivity today was 143% — that doesn’t make sense at all. How can there be more positive results than the number of tests administered? There can’t!
Case positivity cannot be part of the conversation moving forward. The data are clearly inaccurate; the number of cases is clearly an underestimate;
and we know there is community spread of disease.
Let’s agree to not talk about case positivity in 2022.
SO — what should we be using as metrics moving into the new year?
At a community level, we can use continue to use case counts (knowing they are an underestimate of the true amount of disease), the number of hospitalizations, the number of ICU beds available, and mortality (they are all reliable sources of information; however, the data may lag a week or more behind). It would be amazing if we could get data on the number of hospitalized individuals who are vaccinated, who are reinfected, and who have underlying conditions. This would allow us to build a risk profile of what characteristics are associated with severe COVID symptoms. But again, we need to rebuild the public health surveillance system in order to do this at a macro-scale and ensure that the data are valid and reliable.
We can also track the number of individuals who are vaccinated and the number who are boosted. Knowing a breakdown of cases and hospitalizations by vaccination status would also be informative (and possibly helpful as we have conversations with individuals who have not yet received their vaccine).
Communities can also use non-traditional sources of data, such as google trends or the amount of COVID in the sewage. Both of these metrics could be useful in building a narrative around the amount of COVID in a community, but they have countless limitations/drawbacks and must be used with caution. They cannot be used alone (without context or other metrics) to make policy decisions.
Our next right step should be to ensure that our hospitals are not overcrowded with COVID patients. And we should all be working to prevent another death from COVID. Even with Omicron — vaccines are effective at keeping people from developing severe disease and out of the hospital. Everyone should get vaccinated. The virus does NOT care who you voted for or what your political ideology is. It just wants to get into your lungs. The vaccine is NOT aligned with a particular political party or school of thought. It is a public health intervention aimed at protecting you, your family, your friends, and your community.
As we navigate the tightrope in 2022, we must recognize that the world and the virus are changing. And we must adapt. It’s like the wind is changing directions as we are out there on the tightrope. We must adapt and keep moving forward without falling off.
And though one would actually walk on a tightrope individually/alone, let’s all remind ourselves that we are in this together.
Together we are public health.
And soon the fog will clear, the end of the rope will be in sight, and getting to the other end will not feel as challenging as it does today.
