


From Data to Action
Your Guide to Reading the Epidemiological Literature

As a professor of Epidemiology, my primary goal is to teach my students how to read, critically analyze, and apply the results of an epidemiological study to create healthy communities. I want to empower my students to read research papers from beginning to end (not just the Abstract and definitely not skipping the Methods section). I want them to confidently read the literature, determine for themselves the strengths and limitations of the study, and be able to communicate the findings and any applications of those findings to a group of community members without any knowledge of epidemiology.
And I want to invite all of you into my classroom (so to speak). I want to provide you with a guide to reading the epidemiological research and the opportunity to read, discuss, and apply the findings of epidemiological studies with me.
Together — with improved literacy and the ability to see the strengths and limitations that are inherent in every study — we can fight misinformation, spot disinformation, craft strategies to improve health, and create healthy communities.
Are you ready?
If you missed any of the previous posts, you can catch up here:
To wrap up this series, we will be discussing how the epidemiological literature can be used to create public health policy, develop programming, inform health education, and be the foundation for interventions to improve community health.
In short — how can we take the data we’ve collected and analyzed and use it to create healthy communities?
I intentionally put off sharing this post until today because this morning the Supreme Court is hearing oral opening arguments in the abortion medication case. This is a milestone moment in public health and medicine — and waiting for the Supreme Court decision this summer feels like having to wait an eternity.
The Supreme Court weighing in on federal regulatory policies for medications and FDA procedures is a friendly reminder that there is no straight and narrow pathway for moving from epidemiologic data to action. Data collected and conclusions made through epidemiological research must be combined with clinical reports of disease, laboratory results, environmental data, governmental policies, ethical considerations, risk-benefit analyses, and laws/precedents. The picture is complicated — a multiple-circle Venn diagram where many pieces must come together for there to be enough evidence to result in a corresponding change in action.

Infectious Diseases
Let’s first take a look at an infectious disease — one caused by a virus, bacteria, or parasite. In this example, we are going to look at toxic shock syndrome, which is a rare, life-threatening complication of certain types of bacterial infections. Often toxic shock syndrome results from toxins produced by Staphylococcus aureus (staph) bacteria, but the condition may also be caused by toxins produced by group A streptococcus (strep) bacteria.
Epidemiological research published in 1980 concluded that extended use of tampons was causing toxic shock syndrome in menstruating women who used tampons.
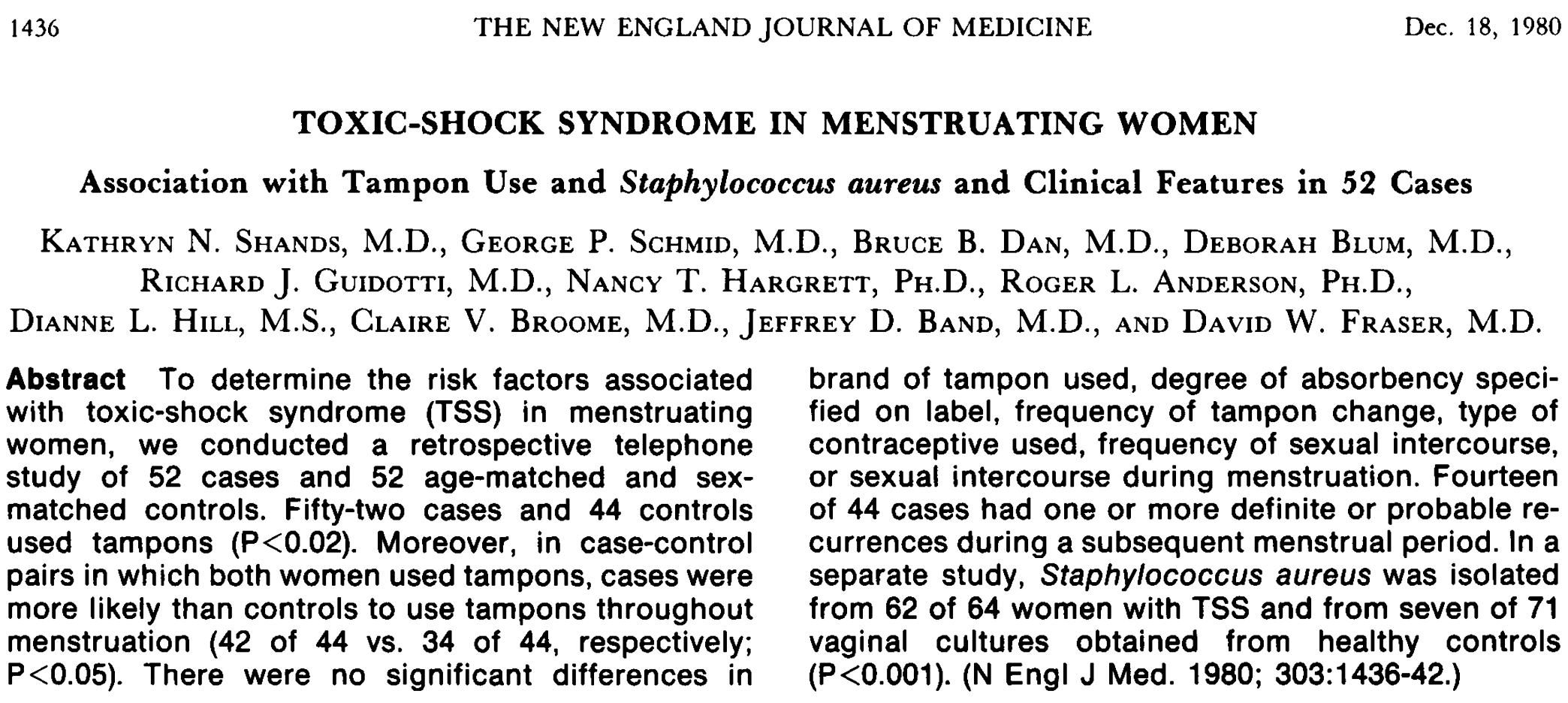
For the federal government to take action — putting warning labels on every box of tampons, warning users of their risk of toxic shock syndrome — not only was an epidemiological study conducted, but a case report was conducted where the clinical manifestation of the disease was documented and associated with extended use of a tampon. Researchers also had to conduct research among different tampon brands to rule out contamination of the tampons themselves as the source of infection.

Four distinct pieces of evidence: (1) epidemiological research; (2) isolation of the staph bacteria from each of the cases; (3) tampon laboratory results; and (4) a clinical case report of a very sick teenage girl was needed to create a clear picture of what was causing women who wore tampons for extended periods of time to contract toxic shock syndrome.
Because we can usually isolate the pathogen causing an infectious disease (even a new pathogen — remember it took the global public health community less than 4 months to identify and map the entire genome of COVID-19), it is possible to move from data to action to stop an infectious disease outbreak if we can identify what the pathogen is, who is getting sick, and under what circumstances or in which environments sickness is occurring.
We call this the infectious disease epidemiologic triangle.

And we can stop the spread of an infectious disease by removing a leg of the triangle. For instance, we can stop a virus with a vaccine. Or slow the spread of the virus in a crowded environment by requiring everyone to wear a mask. Alternatively, we can help individuals who are ill clear a virus with antiviral drugs or an antibiotic.
And then there are non-infectious diseases…
Let’s look at cancer… what CAUSES cancer?
It’s a whole host of things. Genetics, family history, older age, environmental hazards, obesity, smoking cigarettes, drinking too much alcohol, being infected with a virus (HPV or Epstein Barr). Or it could be a combination of all of these things. Ultimately, the cause could be unknown (more to come on all the cancer news among celebrities in the news in a future post…).
After gathering nearly 100 years of medical and epidemiological evidence, the Surgeon General of the United States was able to confidently say that smoking cigarettes increases the risk of all cancers, most notably lung cancer. And action was taken — educational programs were put into place and warning labels were put on cigarette packages.

However, there is not a single, “silver bullet” study that documents that every individual who smokes cigarettes will get lung cancer (they won’t); nor is there a clear threshold or number of cigarettes you can safely smoke and assume that you will not develop cancer. Cigarettes increase cancer risk significantly, but there are still a lot of unanswered questions. Which is why…
It took study after study after study for the world to understand that smoking cigarettes is bad for your health. And is associated with increased cancer risk.
Moving from data to action for a non-infectious disease, such as cancer, requires strategic planning. It requires micro- and macro-level epidemiology. Some researchers need to be out in the field (working at the micro-level) trying to determine what are the risk factors (or the combinations of risk factors) associated with increased cancer risk. Other researchers need to be looking at the canon of cancer epidemiology (at the macro-level) to see what questions remain unanswered and where we are seeing a preponderance of the evidence (where we can begin to say there is evidence to support a conclusion that something(s) might be causing cancer).
When it comes to moving data to action, epidemiological evidence MUST be combined with other forms of evidence — remember, public health is a team sport.
We need laboratory reports to confirm diagnoses.
We need environmental samples to show contamination or exposure to hazards.
We need to rule out other possibilities.
And we need to demonstrate the effectiveness of interventions, such as vaccines, seatbelts, health education programs, access to healthcare, and more.
Epidemiology is an important and (I would argue) foundational tool to understand what is causing disease and then move toward action to disrupt the spread of disease and prevent it from occurring. But epidemiology also relies heavily on the fields of virology, microbiology, vaccinology, environmental health, biostatistics, and clinical medicine.
When we move from doing the research to applying the research — we cannot do so with a single piece of evidence or just one study. We need to accumulate a preponderance of evidence. It is about reading the epidemiological literature AND linking it to the work being done in other fields on the same topic.
Being able to read the epidemiological literature is a great start.
Moving from data to action is next-level. It is taking the appropriate interpretations/conclusions from multiple studies and various points of view and charting the best course of action that aims to create healthy communities for all.
And as we are seeing today in the Supreme Court the pathway from data to action can be challenged legally. Creating, sustaining, and evaluating public health policy to ensure our communities are healthy is hard work. To quote Michael Vaughn from my favorite TV show ALIAS,
“And the work you have ahead of you …
it’s complicated, it’s political, and it is long-term.”
The work we have ahead of us — to create healthy communities for all — is complicated, political, and long-term.
I am so grateful that you are here with me.
I am grateful to you for coming back each week and reading Epi(demiology) Matters.
And I look forward to further discussions about the epi(demiological) news that matters most.
Questions? Thoughts? Comments?
Please share this post (and all the others) with your friends and family —
Epi(demiology) Matters is written by Dr. Becky Dawson, PhD MPH — an epidemiologist, teacher, mom, wife, and dedicated yogi. She is a tenured professor at Allegheny College, Research Director at a community hospital, and an exclusive contributor (all things health & medicine) at Erie News Now (NBC/CBS). Her goal is to create healthy communities for all. She writes Epi Matters — first & foremost because epidemiology does matter (to all of us) and she hopes that each post will help to educate and empower readers to be healthy and create healthy communities.
Be sure you and your friends and family are subscribed so you don’t miss a post —
Epi(demiology) Matters is free — because science, reports, news, updates, and alerts about health should NOT be behind a paywall. EVER. Everyone needs access to up-to-date health information in order to be healthy and create healthy communities for all.