


Mammogram Monday
A day in my life as I completed my annual mammogram

According to the US Preventive Service Task Force, females should start to get an annual mammogram beginning at the age of 40. A mammogram is an X-ray of the breast, and it is a type of screening test — secondary prevention — aimed at identifying breast cancer before there are any signs or symptoms of disease (like a lump). The idea is that a mammogram will discover cancer early in the course of the disease — before a lump can be felt or is noticed. And if the cancer is caught early, it is easier to treat and the outcomes for the individual are much better.
Getting a mammogram is a necessary evil — the procedure is a little uncomfortable and you risk finding out that you have (undetected) breast cancer.
But diagnosing cancer early is essential.
And we need to be talking about mammograms. Friends need to encourage friends to get mammograms. Sons need to check in with their mothers and grandmothers about getting to their annual mammogram appointments. People who love and care for females in their 40s need to talk with them about getting a mammogram every year.
We all need to understand the importance of all females getting an annual mammogram beginning at age 40. We also need to demystify the process of getting a mammogram. We need to make it less scary. And we all need to understand what it means to have a positive screen vs. a negative screen. We all need to understand how screening tests are performed, who needs to be screened, why screening is necessary, and what to do with screening test results.
So come along with me…
Here’s a day in my life as I completed my annual mammogram.
Getting a mammogram, for me, started with my primary care provider (PCP).
Sidebar — pre-COVID I did NOT have a PCP (truth). Finding a provider in a rural community is hard (physicians are not accepting new patients, wait times for appointments are long, and good doctors often leave for jobs in bigger cities). This all changed a couple of years ago; three things coalesced and I prioritized getting a PCP.
First, I developed sepsis in the spring of 2019. And I didn’t have anyone to go to for follow-up visits. I had to assume my infection had cleared; assume my blood work was normal; and assume that the tenderness I felt on my backside was scar tissue, not another budding infection. Combine sepsis with the stress of going up for tenure and then the COVID pandemic, and I knew things were not right physically or mentally. I needed someone to help me navigate high cholesterol, anxiety, and irregular sleep patterns. The third thing was a small miracle — while doing clinical research at the local hospital, I became friends with a sweet doctor, who was about to open her own practice about 20 minutes from my home.
I signed up for my first appointment with Dr. Annie without reservation.
Within a month both of my kids were her patients. And my husband has recently become a patient.
Dr. Annie insisted that I get a mammogram at my first appointment with her.
So my mammograms always begin with her. She writes the order and makes the process of scheduling my mammogram seamless.
I recognize that having a PCP, especially one I truly trust with my life and the lives of my loved ones, is a HUGE privilege.
If you do not have a PCP whom you love, as I love Dr. Annie, know two things —
Taking the time to find a PCP is worth it.
If you are searching (or someone you love is searching) for a PCP and they are a female over 40 years of age, they should not wait to get a mammogram. Here are ways to directly schedule a mammogram without a PCP’s order.
On the day of my mammogram, I showed up and checked in for the procedure. This means getting a wristband.
After check-in, I made my way to the Women’s Center.
After a brief wait, I was greeted by Ashley who took care of me throughout the procedures. First, she had me change into a hospital gown. And I had to remove my deodorant (with baby wipes). Deodorant has to be removed because it can show up as white spots on a mammogram.

Once I was gowned up, I was taken to the mammogram room.


I had two pictures taken on each side of my chest. And yes, getting these pictures taken is a little uncomfortable. The plastic plate (shown in purple below) comes down and spreads the breast tissue out so that accurate pictures can be taken of all of the tissue.

A lot of pressure is applied (think of it as a bowling ball pressing down on your chest).
But the pictures are taken quickly and the uncomfortableness is temporary.
My mammogram was over in 3-4 minutes. And I was in and out of the Women’s Center in 20 minutes. It was a quick and easy cancer screening.
Within 24 hours the results of my mammogram were released.
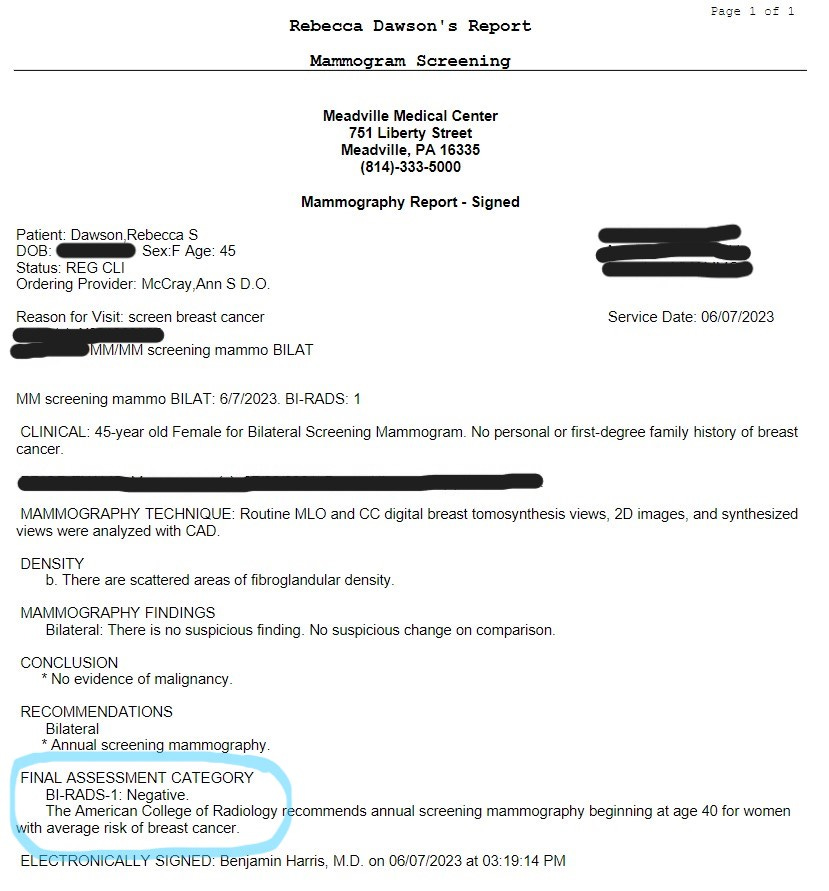
As you can see (section circled in blue), my mammogram was NEGATIVE. This means that there was no evidence of malignancy/cancer. For this, I am truly grateful.
This is my first-ever negative mammogram.
Previously, I had positive mammograms. Meaning that I screened positive — the physician reviewing the X-rays saw something that looked suspicious. So I was called in for further testing. In my case, following a positive mammogram, I had to have a diagnostic ultrasound.
Screening positive does NOT mean you have breast cancer.1
Screening positive means that further testing is needed.
Screening positive is scary.
It takes several weeks for diagnostic testing to be completed and for a clear determination of whether the screen is a true positive (where there actually is cancer) or a false positive (where you screen positive, but there is no cancer). And diagnostic testing requires further medical procedures and extra money.
Screening is imperative.
All females should have an annual mammogram beginning at the age of 40.
The process of being screened for breast cancer through a mammogram takes less than 30 minutes. And while it is temporarily uncomfortable while the X-rays are taken, mammograms are essential. They are able to identify breast cancer before an individual shows symptoms of disease. And early diagnosis leads to improved outcomes for the individual with cancer.
Mammograms are essential.
Questions about mammograms? or breast cancer?
And we all need to be talking about breast cancer — risk factors, screening tests/mammograms, screening test results (a positive mammogram is NOT a good thing), and what to do with the results of a mammogram.

Moving from Meadville to Maine and finding PCP has been a struggle. There are no internal medicine doctors taking patients here. Your option is to see a nurse practitioner, but it will be in six months. David went to see Ryan Landefeld when he was home for Allegheny's graduation and will try the nurse practitioner. I enrolled with a direct primary care physician. Aaron Perreault is amazing. Downside of direct primary care is that it is not covered by insurance. Upside of direct primary care is he is available and responsive.